



In the early 1990s, Pfizer faced a strategic challenge with their newly developed antidepressant, Zoloft (sertraline). At the time, the market for antidepressants was limited by the prevailing view of severe clinical depression as a relatively rare condition. To maximize Zoloft's commercial potential, Pfizer needed to expand the perceived prevalence of depression and, consequently, the pool of potential patients for whom antidepressant medication might be prescribed.
It's not that experiences of low mood or sadness didn't exist prior to the 1990s. Rather, the majority of these experiences were understood as natural, time-limited responses to life events. Most cases of emotional distress were episodic and would resolve on their own without medical intervention. This raised a crucial question for pharmaceutical companies like Pfizer: Why would people turn to a drug for what was largely seen as a normal part of the human experience?
To create a market for antidepressants like Zoloft, it became necessary to shift public perception. The goal was to reframe these common, typically self-resolving mood fluctuations as a medical condition requiring pharmaceutical treatment. This approach would effectively expand the potential customer base beyond the relatively small number of individuals suffering from severe, persistent clinical depression.
This reframing served to blur the lines between ordinary sadness and clinical depression, pathologizing normal emotional responses to life's challenges. By doing so, it created a much larger market for antidepressant medications, even in cases where their necessity or efficacy might be questionable.
In the early 1990s, primary care doctors found themselves at a crossroads when it came to diagnosing and treating depression. These physicians, trained primarily to handle physical ailments, often felt ill-equipped to navigate the complexities of mental health. The prospect of diagnosing depression and prescribing selective serotonin reuptake inhibitors (SSRIs) like Zoloft was met with considerable hesitation and uncertainty.
Several factors contributed to this reluctance. First, there was a pervasive stigma surrounding mental health issues, both in society at large and within the medical community itself. Many doctors worried about labeling patients with a psychiatric diagnosis, fearing it might cause undue distress or social repercussions for their patients.
Moreover, primary care physicians often lacked comprehensive training in psychiatric assessment. The nuanced process of diagnosing depression, distinguishing it from normal sadness or other mental health conditions, seemed daunting to many. Without a clear, standardized approach, doctors feared misdiagnosis or overlooking other potential causes of a patient's symptoms.
The introduction of SSRIs also presented a challenge. While these medications were touted as having fewer side effects than older antidepressants, many primary care doctors felt uncomfortable prescribing psychotropic drugs. They worried about potential adverse effects, drug interactions, and the long-term implications of altering brain chemistry. Some also harbored concerns about the influence of pharmaceutical companies and questioned whether these new drugs were being overpromoted.
Additionally, time constraints in primary care settings made it difficult for doctors to conduct thorough mental health evaluations. The typical 15-minute appointment seemed woefully inadequate for exploring a patient's emotional state, life circumstances, and potential need for antidepressant medication.
Pfizer recognized a golden opportunity to dramatically expand their market for Zoloft by targeting primary care physicians. They understood that if they could normalize the prescription of SSRIs in general practice, they would gain access to a vast pool of potential customers who might never see a psychiatrist. The key was to medicalize depression, transforming it from a severe condition treated by specialists into a common ailment that family doctors could diagnose and treat routinely.
By framing depression as a widespread chemical imbalance rather than a complex psychological state, Pfizer could position Zoloft as a simple, scientific solution. This strategy would not only increase the number of diagnoses but also lower the threshold for what constituted treatable depression. If successful, millions of individuals experiencing normal sadness or temporary mood dips could be recast as patients in need of long-term medication. The potential for profit was enormous, but it required reshaping how primary care doctors - and by extension, the general public - viewed and responded to emotional distress.
The widespread over-diagnosis of depression can be traced back to a marketing ploy by pharmaceutical giant Pfizer.
At the heart of this issue lies the Patient Health Questionnaire-9 (PHQ-9), a deceptively simple screening tool that has reshaped how we view and diagnose mental health.
As revealed in a groundbreaking investigative piece by US health news outlet Stat, the PHQ-9 wasn't born from unbiased scientific inquiry, but from the mind of a marketing executive.
Enter Howard Kroplick, a former marketer for Pfizer, who played a pivotal role in the company's strategy to expand the market for Zoloft. His background in marketing, rather than medicine or scientific research, shaped an approach that would profoundly influence how depression was perceived and treated in primary care settings.

Howard Kroplick
Kroplick recognized that the key to increasing Zoloft prescriptions lay not in traditional advertising, but in changing the very framework within which depression was diagnosed. He proposed the development of a simple screening tool that primary care physicians could easily administer during routine visits. This tool, which would eventually become the PHQ-9, was designed to identify potential cases of depression quickly and efficiently.
The genius of Kroplick's strategy was its dual purpose. On the surface, it provided doctors with a seemingly objective method to assess depression, addressing their hesitation in diagnosing mental health conditions. However, it also served as a powerful marketing tool, effectively expanding the definition of treatable depression and funneling more patients towards antidepressant prescriptions.
By originating from a marketing perspective rather than a purely clinical one, the screening tool prioritized ease of use and broad applicability - factors that would maximize its adoption in primary care and, consequently, expand the potential market for Zoloft.
In essence, the PHQ-9 has reduced the complex spectrum of human emotion to a simplistic checklist, transforming ordinary sadness into a diagnosable - and crucially, medicated - condition. This is not just bad science; it's a calculated strategy that has reshaped our cultural understanding of mental health, all in service of pharmaceutical profits.
While the questionnaire was Kroplick's brainchild, Pfizer shrewdly enlisted respected figures to lend it credibility: psychiatrist Professor Robert Spitzer, clinical psychiatric social work researcher Professor Janet Williams, and primary care clinician Dr. Kurt Kroenke. This veneer of scientific validity masked its true purpose as a marketing tool.
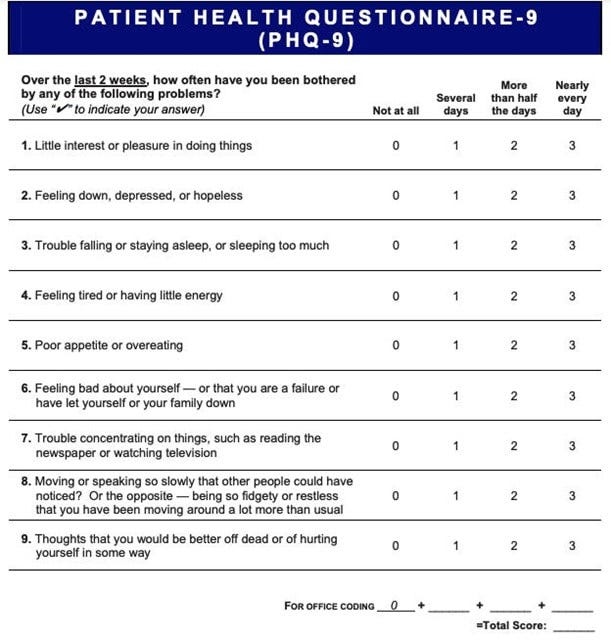
The ramifications of this marketing-driven diagnostic tool are profound and far-reaching. Studies have revealed that the PHQ-9 exhibits a disturbingly high false-positive rate, more than doubling the probability of a depression diagnosis compared to a comprehensive clinical assessment. Examining the questions on the PHQ-9 reveals a troubling lack of context and nuance. These nine items, designed to be universally applicable, capture a wide range of normal human experiences and reactions.
Consider how easily one might endorse feeling "down" or having "little interest or pleasure in doing things" when navigating common life challenges such as job loss, relationship breakups, or the death of a loved one. Sleep disturbances, changes in appetite, and difficulty concentrating are natural responses to stress, yet the PHQ-9 frames these as potential symptoms of a mental disorder.
The questionnaire fails to distinguish between a person grieving a recent loss and someone experiencing clinical depression, or between a student stressed about exams and an individual with a persistent mood disorder. By medicalizing these ordinary reactions to life's ups and downs, the PHQ-9 sets a dangerously low bar for diagnosing depression. This approach not only risks labeling countless individuals with a psychiatric condition they don't have but also trivializes the experiences of those suffering from severe, debilitating depression.
The PHQ-9's stranglehold on mental health screening demands nothing short of a patient rebellion. We must refuse to be reduced to a simplistic nine-question checklist, rejecting this thinly-veiled marketing ploy masquerading as medical care. It's time to challenge our doctors, who've become unwitting pawns in Big Pharma's game, forcing them to confront the flawed foundation of their depression diagnoses. Educate yourself, then educate your physician.
Demand real conversations about your mental state, not cookie-cutter questionnaires. When handed a PHQ-9, tear it up. When pressured to take antidepressants based on a dubious score, push back. This isn't just about individual health - it's about reclaiming our very humanity from the jaws of a system that seeks to pathologize and medicate every flutter of human emotion. The medical establishment won't change unless we force its hand. It's time for mass non-compliance. Only by starving this beast of its data and its docile patients can we hope to dismantle the machinery of overdiagnosis and overmedication.
Your sadness is not a disease.
Your struggle is not a chemical imbalance.
Rise up against the PHQ-9 and reclaim your right to be human.
I wish I’d known how insidious this whole industry was 25 years ago. I lost a huge part of my life to antidepressants.
And if a practice doesn’t give the phq-9 to its patients, it gets financially punished by the insurance companies. It’s all so corrupt.